
Methamphetamine Trends In the United States
Overview
Methamphetamine is a highly addictive central nervous system stimulant that can be injected, snorted, smoked, or ingested orally. Methamphetamine users feel a short yet intense "rush" when the drug is initially administered. The immediate effects of methamphetamine include increased activity and decreased appetite. The drug has limited medical uses for the treatment of narcolepsy, attention deficit disorders, and obesity; however it is seldom prescribed by doctors.
Long-term methamphetamine abuse can cause addiction, anxiety, insomnia, mood disturbances, and violent behavior. Additionally, psychotic symptoms such as paranoia, hallucinations, and delusions can occur. The psychotic symptoms can last for months or years after methamphetamine use has ceased.
Recent Data
The number of domestic lab incidents is increasing at a significant rate in the United States, with the largest increases in the South and Midwest. In March 2009, there were 966 meth lab incidents nationwide, compared to 756 incidents in March 2008 and 596 incidents in March 2007.
In the South, meth lab incidents for Oklahoma, Arkansas, Mississippi, Alabama, and Florida show an increase of 254% from 63 in March 2007 to 223 in March 2009. Methamphetamine labs cost State and local governments significant tax dollars and other resources that could be better spent elsewhere. A study conducted by the independent Rand Corporation in 2009, based on data from 2005, estimated the economic cost to society of methamphetamine use at between $16.2 billion and $48.3 billion. The study found that most of the expenses due to meth use are a result of the “intangible burden that addiction places on dependent users and their premature mortality and from crime and criminal justice costs.”
Meth Lab Incidents Nationwide in 2009
Meth use and meth labs also cause injuries or death to children and public service officials. Environmentally toxic dump sites created by meth labs deflate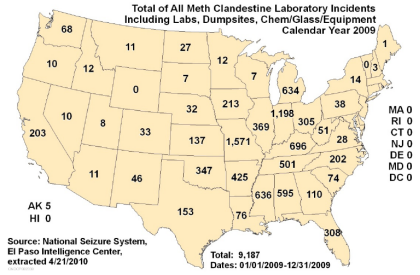 property values and overwhelm medical services, often as a result of uninsured individuals seeking medical help. There are many ingredients used to make methamphetamine, most of which are easily available. One essential ingredient, used by both large and small-scale labs, is pseudoephedrine, found in many cold medications.
property values and overwhelm medical services, often as a result of uninsured individuals seeking medical help. There are many ingredients used to make methamphetamine, most of which are easily available. One essential ingredient, used by both large and small-scale labs, is pseudoephedrine, found in many cold medications.
Federal, State, and Local Responses
In 2005, Congress passed the Combat Methamphetamine Epidemic Act (CMEA), which required that pseudoephedrine (PSE), ephedrine, and phenylpropanolamine5 be placed “behind the counter” and that transaction logs account for sales of these substances from retail outlets. Ephedrine and PSE are precursor chemicals used in the production of methamphetamine. In the CMEA, law enforcement officials were authorized to have access to these logs, and retail outlets were allowed to sell only 3.6 grams of PSE a day per individual purchaser. There appears to be a correlation between the passage of the CMEA and a decrease in meth use in the United States. However, methamphetamine producers have found ways to circumvent the CMEA, and there has been an increase in the number of methamphetamine lab incidents.
State governments, such as those in Oregon and Mississippi, have taken additional steps to address the proliferation of methamphetamine labs in their states. In 2006, Oregon became the first State to require a prescription to purchase pseudoephedrine products, which had been the case Federally before 1976. That year, the Food and Drug Administration approved pseudoephedrine for purchase without a prescription. Mississippi’s State legislature passed the prescription-only law for pseudoephedrine products in 2010; the law takes effect in July 2010. In addition, a few cities in Missouri (including, most recently, Dexter) have also passed laws requiring a prescription for purchase of pseudoephedrine products.
Faced with the limitations of handwritten log books, some States have turned to an electronic log book system. These States, which include Kentucky, Oklahoma, Arkansas, Louisiana, Illinois, Missouri, Kansas, Washington, and Alabama, all have implemented systems to track pseudoephedrine product sales. An individual is asked to provide photo identification before he or she can purchase pseudoephedrine products. If the individual has already reached his or her limit for pseudoephedrine purchases, the sale cannot be made.
Proponents of the tracking system state that thousands of attempted purchases have been blocked, and that electronic tracking has led to 70 percent of the meth lab busts in several Kentucky counties.6 However, critics say the system is easy to circumvent with multiple false identifications. Further, as Kent Shaw, Assistant Chief of the California Department of Justice, Bureau of Narcotic Enforcement, testified before the U.S. Senate Caucus on International Narcotics Control, groups of purchasers can buy enough pseudoephedrine products to fuel large-scale meth “super” labs (clandestine labs that produce 10 pounds or more of methamphetamine in a production cycle). Meth lab incidents in Kentucky have increased from 297 in 2007 to 696 in 2009. Proponents of the electronic tracking system in Kentucky contend that the system needs time to work, and that they are now able to identify the location of more meth labs because of the electronic tracking database.
Results of Oregon Law
Oregon’s prescription-only law has resulted in fewer meth lab incidents in that state. In 2004, according to the El Paso Intelligence Center National (EPIC) Clandestine Laboratory Seizure System, Oregon had approximately 400 lab incidents. In 2008, Oregon had just 20 lab incidents, and most were dump sites found near the borders of adjacent states. Meth-related arrests in Oregon have significantly decreased as well. At the end of 2009, Oregon law enforcement officials made approximately half as many arrests for methamphetamine manufacturing as in late 2006.7 In addition, there have been few consumer complaints regarding the prescription requirement.
Number of Labs Increasing
Despite passage of the CMEA, the number of domestic clandestine meth labs has recently been increasing. Traffickers have adapted to the CMEA and found ways to circumvent the retail sales provisions of the law. Because the CMEA had no provision requiring log books to be electronically connected, traffickers began sending multiple individuals to several retail outlets throughout the day to make single purchases up to the daily limit.
This process, known to law enforcement as “smurfing,” allows criminal groups to obtain large quantities of PSE for methamphetamine manufacturing. Smurfers can purchase multiple packs of PSE for between $7 and $10, then sell the products to lab operators for up to $50 per package.
As with many drugs, there are regional variations in the prevalence of methamphetamine manufacture, distribution, and abuse. Data from the Office of National Drug Control Policy’s Arrestee Drug Abuse Monitoring (ADAM) program show that the percentage of arrestees testing positive for meth is highest in the western region of the country. And California has experienced an increase in “super” labs in recent years, from 10 in 2007 to 15 in 2008 and 13 in 2009.
The Administration’s Efforts to Prevent the Production and Use of Methamphetamine
The Obama Administration is pursuing several efforts to reduce methamphetamine production and trafficking, and to prevent and treat methamphetamine abuse. By emphasizing a balanced approach that recognizes the role of enforcement, as well as prevention and treatment, our 2010 National Drug Control Strategy seeks to reduce the availability and demand for methamphetamine and other drugs.
Specifically, ONDCP’s National Youth Anti-Drug Media Campaign has developed a comprehensive national anti-methamphetamine advertising and public awareness campaign that includes TV, print, radio and online ads, as well as the Web site MethResources,gov, which provides detailed information on meth use, its consequences, and prevention and treatment resources.
The Obama Administration is working to improve intervention and treatment services, particularly by enhancing services delivered by primary healthcare providers. Administration officials are also working with the criminal justice system to reduce methamphetamine-related crime and improve public health and safety. ONDCP funds the National Methamphetamine and Pharmaceuticals Initiative (NMPI), a national effort that serves as a key source of information, coordination, and training to law enforcement officials around the country who are faced with methamphetamine related issues. The 28 designated High Intensity Drug Trafficking Areas (HIDTA) located throughout the country seek to reduce the production, trafficking, and use of methamphetamine. In 2009, HIDTA-funded initiatives were responsible for dismantling nearly 1,400 methamphetamine labs (30 percent of all labs discovered nationwide).
ONDCP is working closely with our partners throughout the Federal Government and Congress, and with State, local and tribal officials to address all aspects of the methamphetamine problem. This dangerous drug poses a serious health and public safety threat, and the Obama Administration is committed to driving down both the consumption and the domestic production of methamphetamine.
Download PDF