
Prescription Drug Monitoring Programs
The abuse of prescription drugs is a serious public health and public safety problem. In 2009, the number of first‐time, non‐medical users of psychotherapeutics (prescription opioid pain relievers, tranquilizers, sedatives, and stimulants) was similar to the number of first‐time marijuana users. The 2010 Monitoring the Future study – a national survey on youth drug use – found that six of the top ten substances used by 12th graders were pharmaceuticals. Further, between 1997 and 2007, treatment admissions for prescription painkillers increased more than four‐fold; over the past five years, the number of emergency room visits involving misuse or abuse of pharmaceuticals doubled, while emergency room visits involving illicit drugs such as heroin and cocaine remained stable. In 17 states and the District of Columbia, drug‐induced deaths are now the leading cause of injury death.
What is a Prescription Drug Monitoring Program (PDMP)? A PDMP is a tool that can be used to address prescription drug diversion and abuse. PDMPs serve multiple functions, including: patient care tool; drug epidemic early warning system; and drug diversion and insurance fraud investigative tool. They help prescribers avoid drug interactions and identify drug‐seeking behaviors or “doctor shopping.” PDMPs can also be used by professional licensing boards to identify clinicians with patterns of inappropriate prescribing and dispensing, and to assist law enforcement in cases of controlled substance diversion.
At the same time, protecting patient privacy is of the utmost importance. PDMPs ensure protection of patient information just as well as, if not better than, any other medical record. Law enforcement may not access patient‐specific PDMP data unless they have an active investigation, and healthcare providers can access only the PDMP data relevant to their patients.
Research Demonstrates PDMP Effectiveness: Several studies show PDMPs are effective when fully utilized. For example, a 2010 study found that when PDMP data were used in an emergency room, 41% of cases had altered prescribing after the clinician reviewed PDMP data – with 61% of the patients receiving fewer or no opioid pain medications than had been originally planned by the physician prior to reviewing the PDMP data, and 39% receiving more opioid medication than previously planned because the physician was able to confirm the patient did not have a recent history of controlled substance use.
Between 2008 and 2009, Wyoming reported a decrease in unsolicited PDMP reports (reports automatically generated when a patient meets or exceeds a threshold for number of prescriptions received) and an increase in solicited PDMP reports (those requested by the prescriber). This combination suggests fewer patients met the criteria for doctor shopping and that prescribers are using the PDMP for its intended purpose. A 2010 independent evaluation of Kentucky’s prescription drug monitoring program, KASPER, found that 90% of those surveyed believed KASPER was effective in preventing drug abuse, diversion, and doctor shopping.
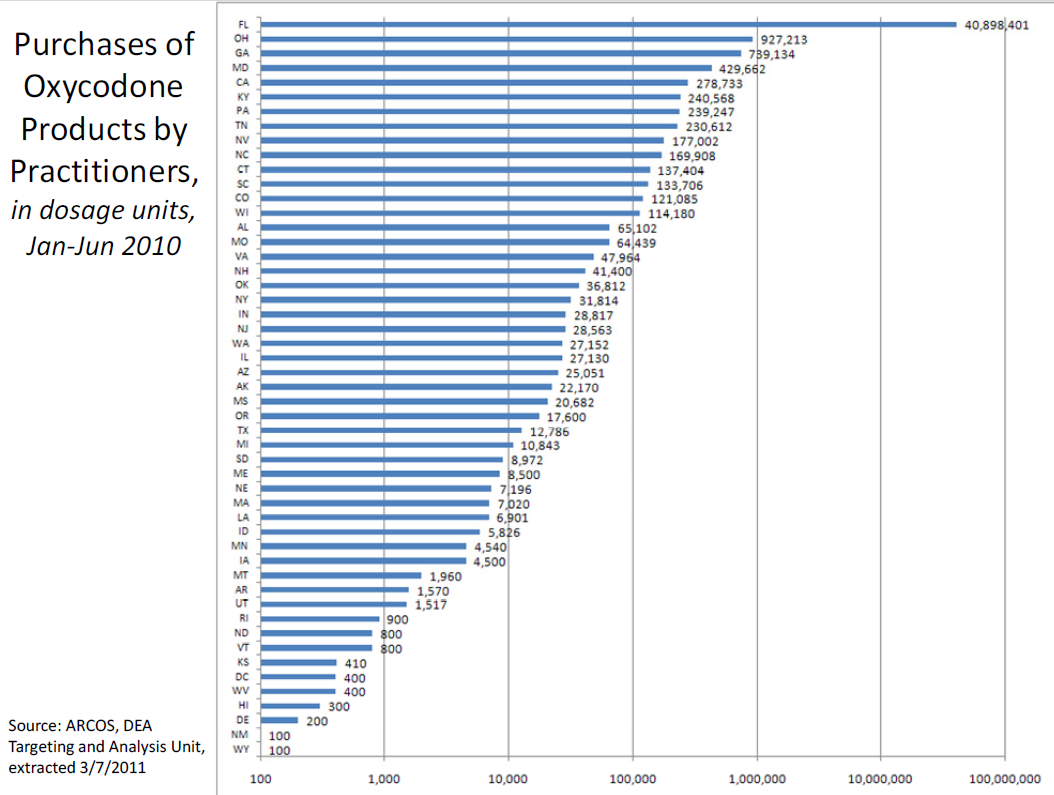
A 2002 GAO report found that Kentucky, Nevada, and Utah reported PDMPs reduced the unwarranted prescribing and subsequent diversion of abused prescription drugs in their states. Of the ten states with the highest number of prescriptions for OxyContin, only two had PDMPs; six of the ten states with the lowest number of OxyContin prescriptions had PDMPs. The chart on page 3 shows the states rankordered according to the purchases of oxycodone products by practitioners in the first half of 2010. Florida, which does not have an active PDMP, leads the country in such purchases, with more than 40 times as many as the next‐leading state, Ohio. (Note: the chart uses a logarithmic scale to display the data in order to depict Florida’s high number of purchases on the same chart as the other states.)
Why the Expansion of PDMPs Makes Sense: Currently, 35 states have operational PDMPs, and 11 additional states and 1 U.S. territory have passed legislation authorizing the development of a PDMP. Because not all states have a PDMP, and because data sharing and interoperability between states has not been implemented, the full benefit of PDMPs has not been realized.
ONDCP is aggressively working with Federal, state, and non‐governmental partners to support the development of operational PDMPs in every state. The programs would be used in clinical practice and have the ability to share data with PDMPs in other states. Incorporating PDMPs into a comprehensive prescription drug diversion and abuse prevention strategy that includes education for healthcare providers, patients, and the public on prescription drug abuse; consumer‐friendly, environmentally responsible medication‐disposal programs; and smart law enforcement aimed at reducing pill mills and doctor shopping, can reduce the consequences of prescription drug abuse in our Nation.
Download PDF