
US Demand Reduction Efforts
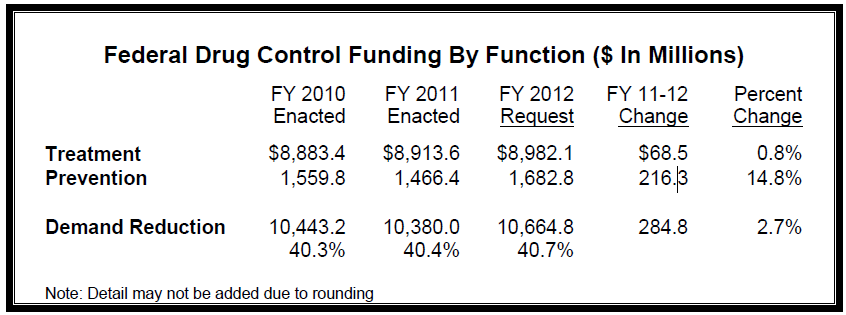
The United States is dedicated to a comprehensive, balanced approach of prevention, treatment, and enforcement. This document provides information about ONDCP’s efforts to prevent drug use and treat addiction. In FY 2012, the Obama Administration requests approximately $10.7 billion to support demand reduction. This includes a nearly 15 percent increase for prevention, and a 1 percent increase for treatment over the FY 2011 enacted level. The overall FY 2012 national drug budget request, including supply reduction, is $26.2 billion, an increase of $485.7 million over FY 2011.
Drug Use in America
In 2009, an estimated 22 million Americans aged 12 or older were current (past month) illicit drug users.
- Drugs most used include marijuana/hashish, cocaine (including crack), heroin, hallucinogens, inhalants, and prescriptiontype psychotherapeutics. Marijuana and pain relievers are the drugs of choice for new users. In 2009, an estimated 3.1 million persons aged 12 or older used an illicit drug for the first time. Most in that group used marijuana (59.1 percent) and pain relievers (17.1 percent).
- Drugs caused more deaths than firearms and alcohol in 2007. According to the Centers for Disease Control and Prevention, 38,371 people died of drug‐induced causes in 2007, the latest year for which data are available. This compares with 31,224 deaths from firearms injuries and 23,199 alcohol‐induced deaths.
Prevention
- Prevention is most successful when messages are conveyed at home (core values) and reinforced in schools, workplaces, and community organizations (reinforcing values). They should link prevention and overall health, reflecting shared social norms (prevailing values).
- Prevention-Prepared Communities: The FY 2012 request includes $15.0 million for a pilot network of “prevention‐prepared communities.” These offer continuous evidence‐based interventions throughout adolescence. $5.6 million is requested for community specialists to develop prevention‐prepared communities and increase state agency collaboration. Activities include state‐level drug monitoring, technical assistance, and mentoring networks. Also, $2.0 million is requested to fund evaluations of the pilot program.
- State Substance Abuse Prevention Grants. The FY 2012 request includes $395.0 million for a new state formula grant for substance abuse prevention. This new grant program combines legacy funding from the Strategic Prevention Framework program and the Prevention set‐aside from the Substance Abuse Prevention and Treatment Block Grant to fund state‐supported, evidence‐based community prevention programs.
- The National Youth AntiDrug Media Campaign. The FY 2012 request of $45.0 million targets youth and their parents through advertising and public outreach on television, radio, in magazines and on the Internet. For more information, visit online: www.TheAntidrug.com.
- Drug Free Communities (DFC) Support Program. The FY 2012 request of $88.6 million for DFC provides grants of up to $125,000 per year, for a maximum of 10 years, to local coalitions to mobilize communities against drugs. Community coalitions strive to develop local solutions and increase community involvement and effectiveness in carrying out a wide array of drug prevention strategies, initiatives, and activities. For more information go to: www.ondcp.gov/dfc.
- Successful, Safe, and Healthy Students. Education requests $266.9 million in FY 2012 for a new program that supports student achievement and helps ensure students are mentally and physically healthy and ready to learn. The objective is to create an improved school climate that reduces drug use, violence, and harassment and improves school safety and students’ physical and mental well‐being.
- Drugged Driving. The National Highway Traffic Safety Administration’s FY 2012 $2.8 million request will support the Drug‐Impaired Driving Program, which will provide public information, outreach efforts, and improved law enforcement training to help reduce drugged driving. Funding will also support a new roadside survey of drug use by drivers and completion of a study of the crash risk of driving after taking drugs.
Treatment
- Substance Abuse Treatment block grant. $1.5 billion is requested to support the public health systems provision of treatment services to those suffering from addiction. This formula‐based funding to states expands substance abuse treatment services, while providing maximum flexibility to states.
- Grants to states for Medicaid funded treatment. Substance abuse treatment most often is paid for by two or more public and private sources (private health insurance, Medicaid, Medicare, state and local funds, and other Federal support). ONDCP’s estimated share of the Federal Medicaid expenditures for substance abuse treatment is $3.6 billion.
- Medicare funded treatment. Medicare‐funded substance abuse treatment is an entitlement for eligible Medicare participants, estimated at $1.6 billion in FY 2012. Coverage and costs are increasing with the growing demand for treatment and the addition of Part D coverage prescription drug coverage.
- Screening, Brief Intervention, and Referral to Treatment (SBIRT). SBIRT is a low‐cost, high‐impact approach whereby patients receiving medical services in regular health facilities are screened for drug abuse and referred to follow‐up treatment, if necessary. The FY 2012 request through the Substance Abuse and Mental Health Services Administration (SAMHSA) is $27.1 million. By October 2010, 1.2 million patients in grantee sites had been screened: 14.8 percent required brief interventions, 2.4 percent required brief treatment, and 3.1 percent required referrals to specialized programs. More information is available online at www.sbirt.samhsa.gov/about.htm.
- Drug Courts. In FY 2012, the Justice Department requests $57.0 million for support to Drug Courts, providing grants to criminal justice agencies to implement and improve drug court programs. SAMHSA’s FY 2012 request of $43.8 million will provide services to support substance abuse treatment, assessment, case management, and program coordination for those in need of treatment services. Drug Courts serve 44.7 percent of counties in the U.S. They reduce recidivism, longterm costs, and drug demand.
- Research on diversion strategies: The Department of Justice’s FY 2012 request of $10.0 million builds on the work of Drug Courts, community supervision of offenders, and other offender diversion strategies to develop, test, and evaluate the next generation of cost‐effective diversion programs.
- ExOffender Reentry program grants. The FY 2012 request includes $22.6 million for SAMHSA’s Ex‐Offender Reentry program grants, which provide screening, assessment, and comprehensive treatment and recovery support services to offenders reentering the community, as well as to offenders who are currently on or being released from probation or parole.
- Residential Substance Abuse Treatment (RSAT). $30.0 million requested for RSAT supports the provision of residential treatment prior to release in state and local prisons and jails.
- Bureau of Prisons drug treatment efforts. The Violent Crime Control and Law Enforcement Act of 1994 requires the Bureau of Prisons to provide residential substance abuse treatment to all eligible inmates. The FY 2012 request of $108.5 million will allow for the expansion of drug treatment capacity.
- Substance Abuse Treatment for Veterans. With its $541.7 million FY 2012 request, the Veterans Health Administration (VHA) operates a national network of substance abuse treatment programs located in medical centers, residential rehabilitation facilities, and outpatient clinics. In light of the frequent co‐occurrence of substance use disorder problems with Post Traumatic Stress Disorder (PTSD), VHA is also assigning a full‐time substance use disorder specialist to each of its hospital‐level PTSD services or teams.
Recovery Support
Coordinated after‐care, peer‐led support, and other recovery support services help people build or re‐build a lifestyle of health and wellness in addition to non‐use. Effective recovery support programs also help people gain skills that lead to self‐sufficient and productive lives without using substances.
- The Second Chance Act shifts priority to rehabilitating parolees. Re‐entry programs combine treatment, job training, employment assistance, and life skills training. Long‐term treatment is available upon release. $50.0 million of the funding requested for Second Chance Act programs is scored for budget purposes as drugrelated. Additionally, the Administration supports drug testing and sanctions for violations, approaches that have been shown to deter drug use and re‐incarceration among the community correctional population.
- Access to Recovery enables treatmentseeking populations to choose their preferred treatment modality and ancillary services. Through an individualized assessment and voucher system, comprehensive services are provided, ranging from housing, job training, and relapse prevention to childcare and transportation. The FY 2012 Budget requests $98.5 million to support selected ongoing programs and approximately 30 new grants. More information is available online at: www.atr.samhsa.gov.
Download PDF