ONDCP Blog
Expansion of Innovative Law Enforcement Collaboration
Posted by on November 14, 2013 at 11:04 AM ESTToday, Director Kerlikowske announced the expansion of an innovative law enforcement program that fosters collaboration between Federal, state, local and tribal law enforcement officers. The High Intensity Drug Trafficking Areas (HIDTAs) program has recently added 12 new counties in nine states, enabling those counties to receive Federal resources to facilitate cooperation, information sharing and coordination across organizational lines. See a list of the newly designated counties here.
The HIDTA program was created by Congress with the Anti-Drug Abuse Act of 1988 to support coordinated law enforcement efforts to reduce the supply of illegal drugs—in areas designated “high traffic” and across the Nation. In 2012 alone, HIDTAs collectively disrupted/dismantled 3,033 drug trafficking organizations, removed over $17.8 billion worth of drugs, and seized over $1.9 billion in cash and assets.
In addition to designating 12 new counties, Director Kerlikowske also announced nearly $3 million in discretionary funding to 21 HIDTAs to enhance targeted enforcement and drug prevention efforts nationwide. The discretionary funds will support strategic priorities based on the unique threats in each HIDTA, including prescription drug abuse and synthetic drugs.
Leveraging the latest technology and counter-terrorism expertise—and defined by the spirit of collaboration—HIDTAs are a national model for effective cross-agency partnerships. Learn more about HIDTA accomplishments here.
Learn more aboutRemembering our colleague, Ed Jurith
Posted by on November 12, 2013 at 3:38 PM EST
It is with great sadness that today we announce the passing of our beloved colleague, Ed Jurith. During his distinguished career at the Office of National Drug Control Policy (ONDCP), Mr. Jurith was appointed twice to serve as Acting Director—first by President Clinton in 2001, then by President Obama in 2009. Since 1994, he also served as ONDCP’s General Counsel, Senior Counsel and Director of Legislative Affairs.
With his characteristic intelligence, deep insight and good humor, Mr. Jurith embodied the best of public service. He was one of the brightest minds in drug policy, with more than 30 years of Federal policy-making experience. He came to ONDCP from the U.S. House of Representatives, Select Committee on Narcotics Abuse and Control, where Mr. Jurith was Staff Director from 1987 to 1993 and Counsel for five years prior to that. While on staff at the Select Committee, he was instrumental in the development of the Anti-Drug Abuse Acts of 1986 and 1988—which set the framework for U.S. drug policy, and established this very office 25 years ago.
Mr. Jurith’s reputation as a leader in drug policy crossed international borders. In 1997, he served as an Atlantic Fellow in Public Policy at the University of Manchester in the United Kingdom, where he researched and lectured on drug policy issues. As part of the Atlantic Fellowship, Mr. Jurith assisted the UK Anti-Drugs Coordinator in the development of the Blair government’s strategy for reducing substance use. He lectured widely on drug policy at U.S. and British universities and authored numerous publications in the arena of substance abuse and drug policy. In addition, Mr. Jurith represented the United States on the board of the World Anti-Doping Agency for many years.
Back home, in 2010 he became an adjunct professor at the American University Washington College of Law, where he taught a seminar on the intersection of law and drug policy. His class was extremely popular—enrollment in Mr. Jurith’s course increased from seven students in its first year to capacity (plus a wait list) in the second year. In the words of the College of Law’s Associate Dean for Student Affairs, students found him both engaging in the classroom and interested in their professional development outside the classroom.
Prior to his federal government service, Mr. Jurith was an attorney in private practice in his native New York City. He graduated, cum laude, from American University in 1973 and received a Juris Doctor from Brooklyn Law School in 1976. As a member of the New York, District of Columbia and U.S. Supreme Court Bars, Mr. Jurith served on the Advisory Committee of the American Bar Association Standing Committee on Substance Abuse, as well as the District of Columbia Bar Lawyer Assistance Program, a program providing assistance to law students, lawyers and judges with substance use and/or mental health disorders.
Mr. Jurith is survived by his wife, Kathleen Healy, and his sons Theodore and William. We keep his family in our thoughts and prayers, and honor Ed’s memory by renewing our commitment to the crucial work to which he dedicated his career.
Learn more aboutA Veterans Day Message
Posted by on November 8, 2013 at 6:01 PM ESTThis Veterans Day, we join President Obama, the U.S. Department of Veterans Affairs (VA), and the entire country in honoring our Nation’s veterans. Since the dawn of our country, these brave men and women have fought for and protected the freedoms that make America great. We owe them our deepest gratitude all year round, but today, in particular, we pause to thank them for their selflessness and their service.
There are many ways to honor and thank all who served in the United States Armed Forces this Veterans Day. Join a ceremony near you, and lend your voice online to a simple message of thanks on social media. The VA offers a variety of web-based and phone services online, particularly for veterans in need of mental health services. Visit this page for more information.
Here at the Office of National Drug Control Policy, we are proud to work alongside veterans who lend their talent and energy to the important task of reducing drug use and its consequences across the country. Before he led ONDCP or the Seattle and Buffalo police departments, Director Gil Kerlikowske served in the United State Army, where he was awarded the Presidential Service Badge.
This weekend, we honor our ONDCP leadership and staff who have served proudly, as well as the millions of veterans across the Nation.
Learn more aboutEnding Discrimination and Opening the Doors to Treatment: Drug Policy Reform
Posted by on November 8, 2013 at 11:11 AM ESTToday, Director Kerlikowske joins the Departments of Health and Human Services, Labor, Treasury, and the Office of the Vice President in announcing the final rules providing equal coverage or parity for individuals needing treatment for mental health or substance use disorders and who are covered by group and individual health plans.
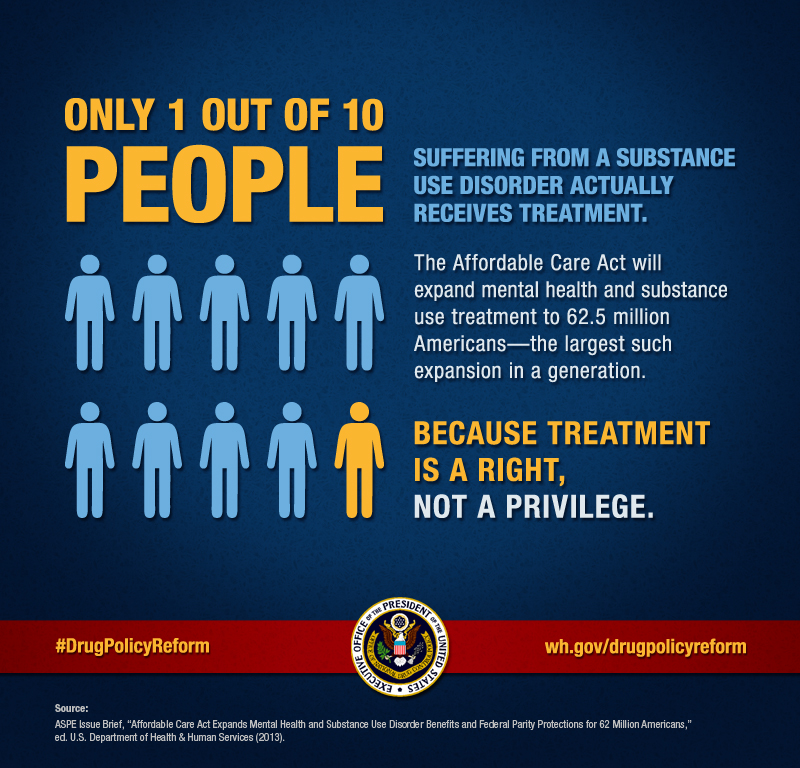
Substance use disorders are treatable—and recovery is possible—but too many Americans have not been able to get treatment because they didn’t have insurance coverage for treatment services. According to the 2012 National Survey on Drug Use and Health, about 23 million Americans were in need of treatment for a substance use disorder, and only 2.5 million—about 1-in-10—actually received needed treatment.
Today’s rule, made possible by the Mental Health Parity and Addiction Equity Act (Parity Act) makes it easier for those Americans to get the care they need by ending discriminatory practices that limited insurance coverage for behavioral health treatment and services. The Affordable Care Act (ACA) extends the reach of the Parity Act’s requirements. Starting in 2014, the ACA will require all small group and individual market plans created before March 23, 2010 to comply with federal parity requirements. Qualified Health Plans offered through the Health Insurance Marketplaces in every state must include coverage for mental health and substance use disorders as an Essential Health Benefit, and that coverage must comply with the federal parity requirements set forth in MHPAEA.
One of the most significant pieces of drug policy reform in a generation, this rule will expand mental health and substance use disorder services to 62 million Americans. This builds on the historic momentum we’ve achieved toward treating our nation’s drug problem as a public health issue, not just a criminal justice issue. For decades, science has shown us that addiction is a chronic disease of the brain that can be successfully prevented and treated - not a moral failure on the part of the individual.
Today, we honor that research by ensuring that our healthcare system provides the same level of medical coverage for substance use disorders as it does for other chronic diseases, like cancer or diabetes.
Learn more aboutA Different Kind of Birthday
Posted by on November 4, 2013 at 3:51 PM ESTToday marks 25 years since I started my journey of recovery.
Coincidentally, the same year I started that journey—in fact, the very same month—a law was created to establish the office where I now serve President Obama.

Photo: Deputy Director Botticelli addressing a group of new American citizens at their naturalization ceremony.
I know that today is just another day, but it is a day filled with joy and gratitude as I think about how my life has changed. While I am so grateful for the opportunities my recovery has given me, it is really the profound internal changes that matter most. I am not the person I was 25 ago. Some parts of the country refer to these milestones as “birthdays,” which is very appropriate given that recovery means a chance at a new life filled with meaning, purpose, joy and love. As I have often said, my story is not unique. I am one of millions of Americans who found a way back from the grip of addiction through the kindness and caring of many, many people.
Like many people with addictions, one of the biggest obstacles I faced in asking for help was that I could not imagine a life without drinking. Even though my life was a disaster, I could not see how stopping would lead to a happy and fulfilling life. What would people think of me if I said I had an addiction? What would my boss think? Would I ever have a social life again filled with friends? I did not see people like me living a happy life in recovery.
I can’t help but think that the recent Supreme Court rulings on gay marriage were in large part driven by the simple, yet courageous act of gay men and lesbians coming out to their family, friends, neighbors and co-workers. It changed public opinion and drove public policy. The same was true with people with HIV and even people with cancer faced fear, shame and stigma. When Magic Johnson announced that he was HIV positive, there was a significant increase in the number of people getting tested. ACT Up demanded expedited research and drug approval, funding for services and a compassionate response by the medical community. Any great movement to change public perception and public policy has often been fueled by people who are affected “coming out” of the shroud of secrecy and invisibility.
Photo: Deputy Director Botticelli representing ONDCP at the West Virginia Behavioral Health Conference.
Yet, for too many people and their families, asking for help and seeking care for a substance use disorder is still saturated with shame. Despite the fact that nearly every family and community in America is affected by addiction, it remains part of our collective denial. According to the National Survey on Drug Use and Health, only about 1 in 10 people with a diagnosable substance use disorder get treatment at a specialty facility. Compare this to diabetes where the treatment rate is 84%[1]. For those who do get treatment, it is often in the most acute stages where, even though effective, treatment is more challenging and costly. The economic cost of excessive alcohol use is estimated to be $223 billion, with health care accounting for $24.6 billion of these costs.[2] The economic cost of illicit drug use is estimated to be $197 billion, with health care accounting for $11.4 billion of these costs.[3] None of these figures compare to the pain, anguish and grief addiction causes.
Decades of scientific research have given us an irrefutable understanding of addiction as a health issue, a chronic medical condition with genetic, biologic and environmental risk factors. It requires a comprehensive public health approach using evidenced-based prevention, early intervention, treatment and recovery support services. The 2013 National Drug Control Strategy, the Obama Administration’s blueprint for drug policy, is based on this understanding. It puts forth more than 100 action items across federal government to prevent drug use and its consequences. It dismisses a “war on drugs” approach, while acknowledging the vital role that federal, state and local law enforcement play in reducing the supply of drugs. With a public health framework at its foundation, the Strategy sets forth an agenda that tackles systemic challenges like over-criminalization, lack of integration with mainstream medical care, insurance coverage and legal barriers to fully restoring people to productive and meaningful lives. The implementation of the Affordable Care Act addresses some of these systemic issues by dramatically increasing coverage for treatment and ensuring that services are comparable to other chronic conditions for over 62 million Americans.
All of these advancements, however, are not enough unless we fundamentally change the way many people think about addiction. The Parternship at DrugFree.org and The New York State Office of Alcoholism and Substance Abuse Services (OASAS) estimate that there are more than 23 million individuals in recovery. Millions of people in recovery are living meaningful, productive lives full of joy and love and laughter—and I am just one of them. It is time for those of us in recovery, and those that care for and love us, to join the growing movement to put a face and voice to this disease; to lift the curtain of invisibility and to show others the endless possibilities of a life in recovery.
It is a time to make that simple, yet courageous decision to be counted, to be seen and to be heard.
Michael Botticelli is the Deputy Director of National Drug Control Policy.
[1] Centers for Disease Control and Prevention. National Diabetes Fact Sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011.
[2] Bochery, EE et al., 2011. Economic costs of excessive alcohol consumption in the U.S., 2006. American J. Preventive Medicine 41(5):516-524.
[3] National Drug Intelligence Center. 2010. National Threat Assessment: The Economic Impact of Illicit Drug Use on American Society. Department of Justice, Washington, DC.
Learn more aboutOctober is National Substance Abuse Prevention Month
Posted by on October 22, 2013 at 4:02 PM ESTWhile substance use prevention is a year-round prioirity, during the month of October, the Office of National Drug Control Policy highlights and joins substance use prevention efforts across the country as part of National Substance Abuse Prevention Month.
Learn more about National Substance Abuse Prevention Month and read the Presidential Proclamation.
Learn more aboutNotice
Posted by on October 1, 2013 at 8:54 AM ESTDue to Congress’s failure to pass legislation to fund the government, the information on this site may not be up to date. Some submissions may not be processed, and we may not be able to respond to your inquiries.
The ONDCP blog will not be updated during the lapse in funding.
Information about government operating status and resumption of normal operations is available at USA.GOV.
Learn more aboutInnovation in Substance Use Disorders and Mental Health Treatment
Posted by on September 16, 2013 at 4:47 PM ESTToday, the Office of National Drug Control Policy hosted a conference at the White House to highlight innovative technologies for substance abuse treatment, wellness, mental and behavioral health. Supported by the Substance Abuse and Mental Health Administration (SAMHSA), the Office of National Coordinator for Health Information Technology (ONC), and the Office of Science and Technology Policy (OSTP), the conference was kicked off by U.S. Chief Technology Officer Todd Park and Office of National Drug Control Policy Director Gil Kerlikowske.

Mr. Park previously served as Chief Technology Officer of the U.S. Department of Health and Human Services, where he helped HHS harness the power of data, technology, and innovation to improve the health of the Nation.
Conference panelists presented on a range of innovative health technologies—from smartphone apps that help people stay sober to biosensors that can detect human emotion. You can find the full conference agenda online here and archived video of the conference will be available here.
During the conference, ONC’s Jodi Daniel announced the winner of the Behavioral Health Patient Empowerment Challenge, the Hazelden Foundation's Mobile MORE smartphone app. We congratulate Hazelden and thank all conference participants for a lively, engaging day discussing some of the most forward-leaning innovations in behavioral health.
Search for the hashtag #InnovateBH on Twitter to see more from today's conference.
Learn more aboutSubstance Abuse Prevention is Suicide Prevention
Posted by on September 10, 2013 at 3:41 PM ESTWhen we prevent or successfully treat substance abuse, we prevent suicides. There is a powerful connection between the missions of the substance abuse prevention and treatment communities and the suicide prevention community – and much to be gained when these groups come together around their common goals.
Drug poisoning deaths have increased 120 percent in recent years – from 17,415 in 2000 to 38,329 in 2010. The majority (58 percent) of the drug deaths involved pharmaceuticals, and 75 percent of those deaths involved prescription pain relievers.[i] In 2010, U.S. emergency departments treated 202,000 suicide attempts in which prescription drugs were used as the means, 33,000 of which were narcotic pain relievers.[ii]
The suicide and substance abuse prevention fields need to align their efforts to promote healthy individuals and healthy communities.
Many of the factors that increase the risk for substance abuse, such as traumatic experiences, also increase the risk for suicidal thoughts and behaviors,[iii],[iv] and substance abuse, like mental health problems, is linked with a several-fold increase in suicide risk.[v],[vi]
There is hope, however: Prevention works, treatment is effective, and recovery is possible. Life skills that support effective problem-solving and emotional regulation, connections with positive friends and family members, and social support can protect individuals from both substance abuse and suicide. Treatment and support are important precursors for recovery from substance abuse as well as recovery from suicidal thoughts.[vii],[viii]
In September 2012, a newly revised National Strategy for Suicide Prevention (NSSP) was released by the National Action Alliance for Suicide Prevention (Action Alliance) in conjunction with the Office of the Surgeon General. The Action Alliance is a public-private partnership, jointly launched in 2010 by the Secretaries of Health and Human Services and Defense, envisioning a Nation free from the tragic experience of suicide. The connection between suicide prevention and the prevention and treatment of substance abuse is either implicit or explicit in each of the 13 goals of the NSSP, as it should be. Recognizing this, the NSSP calls for several actions, including:
- Train staff in substance abuse treatment settings to ask their clients and patients directly and in a non-judgmental way whether they are having thoughts of suicide or think things would be better if they were dead. Ask on intake and periodically throughout the course of treatment, and ask in a way that opens the door for a truthful response.
- Work with individuals, families and other social groups, and communities to reduce access to drugs, especially access to lethal quantities of drugs among individuals at increased risk for suicide. This includes reducing stocks of medications kept in the home, locking up commonly abused medications, and encouraging the proper disposal of unused and unneeded prescription drugs, a key component of the 2013 National Drug Control Strategy.
Let us commit to stronger collaboration between substance abuse and suicide prevention efforts at all levels: community, state, tribal, and national. And let’s take action. The stakes are too high to do otherwise.
Dr. Litts is the Executive Secretary for the National Action Alliance for Suicide Prevention. Previously, David held a variety of leadership positions in the Nation’s suicide prevention movement, including the Air Force’s pioneer suicide prevention program (1996-1999) and development of the 2001 National Strategy for Suicide Prevention.
Ms. Carr is a Senior Policy Analyst with the National Action Alliance for Suicide Prevention. Previously, she was the Suicide Prevention Specialist for the Massachusetts Department of Public Health and the Education Coordinator for the Massachusetts/Rhode Island Regional Center for Poison Control and Prevention.
The National Action Alliance for Suicide Prevention is the public-private partnership advancing the National Strategy for Suicide Prevention (NSSP) by championing suicide prevention as a national priority, catalyzing efforts to implement high priority objectives of the NSSP, and cultivating the resources needed to sustain progress.
[i] Centers for Disease Control and Prevention. National Vital Statistics System. 2010 Multiple Cause of Death File. Hyattsville, MD: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2012.
[iii] Dube, S, Felitti V et all. (2003). Childhood Abuse, Neglect, and Household Dysfunction and the Risk of Illicit Drug Use: The Adverse Childhood Experiences Study. Pediatrics, Vol. 111 No. 3.
[iv] Afifi T, Murray W, et al. (2008) Population Attributable Fractions of Psychiatric Disorders and Suicide Ideation and Attempts Associated With Adverse Childhood Experiences. American Journal of Public Health 2008, Voi 98, No. 5.
[v] Conwell Y, Duberstein PR, Cox C, Herrmann JH, Forbest NT, Caine ED (1996). Relationships of age and axis I diagnoses in victims of completed suicide: A psychological autopsy study. American Journal of Psychiatry, 153(8): 1001-1008.
[vi] Moscicki EK (2001). Epidemiology of completed and attempted suicide: Toward a framework for prevention. Clinical Neuroscience Research, 1, 310-323.
[vii] Brown, G. K., Ten Have, T., Henriques, G. R., Xie, S. X., Hollander, J. E., & Beck, A. T. (2005). Cognitive Therapy for the Prevention of Suicide Attempts: A Randomized Controlled Trial. JAMA: Journal of the American Medical Association, 294(5), 563-570.
[viii] Linehan, M. M., Comtois, K. A., Murray, A. M., Brown, M. Z., Gallop, R. J., Heard, H. L., et al. (2006). Two-Year Randomized Controlled Trial and Follow-up of Dialectical Behavior Therapy vs Therapy by Experts for Suicidal Behaviors and Borderline Personality Disorder. Archives of General Psychiatry, 63(7), 757-766.
Learn more aboutAnnouncing the Opioid Overdose Toolkit
Posted by on August 28, 2013 at 10:32 AM ESTApproximately 100 Americans died from overdose every day in 2010. In just one year, we lost 38,000 people to overdose—more than the number who died from either homicides or traffic crashes. 22,000 of those deaths involved prescription drugs, and more than 3,000 involved heroin. Frighteningly, other data show that opiate use among young people is increasing.
These numbers are staggering. Here’s what makes them heartbreaking: every overdose death is preventable. Two years ago, we released a comprehensive plan to address our nation’s prescription drug abuse epidemic. This plan supports prescription drug monitoring programs, convenient and environmentally responsible drug disposal methods, education for patients and prescribers, and law enforcement efforts to decrease diversion of prescription drugs.
In honor of International Overdose Awareness Day, this Saturday, August 31, we are joining other federal partners to announce the release of the Opioid Overdose Toolkit. The Toolkit, developed by the Department of Health and Human Services, provides information on overdose prevention, treatment and recovery for first responders, prescribers, and patients.
This toolkit builds upon our efforts to expand prevention and treatment. It also promotes the use of naloxone, a life-saving overdose reversal drug which we believe should be in the patrol cars of every law enforcement professional across the nation. We have lost too many loved ones to overdose, and the deadly disease of addiction has remained for too long in the shadows. It is time to speak out. By raising awareness, we can honor those we’ve lost by preventing future losses.
Get the facts on preventing, treating and surviving overdose.
Michael Botticelli is the Deputy Director of National Drug Control Policy.
Learn more about
- &lsaquo previous
- …
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- …
- next &rsaquo