ONDCP Blog
Fostering Our Tribal Youth and Building Healthier Communities
Posted by on August 7, 2015 at 10:46 AM EST At the annual United National Indian Tribal Youth (UNITY) conference, tribal youth engaged senior Administration officials on issues affecting their communities. Many conference participants voiced concern about illicit substance use among their peers. A substantial portion of the American Indian and Alaska Native population is under the age of 24 (42 percent compared to 34 percent of the general population), and a significant percentage of the population falls in the 15-19 age group. Young people are our Nation’s greatest resource, so it is essential that we do everything we can to encourage healthy, drug-free youth communities in Indian Country. One of the conference participants was Margarita, a member of the Ute Mountain Ute Tribal Youth Task Force Coalition, which is a community coalition sponsored by the Drug-Free Communities (DFC) Support Program. This coalition is one of the many examples of how the DFC program is helping to build healthy tribal communities. How has the program grant helped her community? “DFC has played an important role,” said Margarita. “I don’t think the adults know what problems youth are facing because they are not youth anymore. Having young people at the table gives them the advantage to know, ‘okay, this youth said this isn’t a good idea, so maybe we should take a different approach in fighting the battle against substance use.’ ”
At the annual United National Indian Tribal Youth (UNITY) conference, tribal youth engaged senior Administration officials on issues affecting their communities. Many conference participants voiced concern about illicit substance use among their peers. A substantial portion of the American Indian and Alaska Native population is under the age of 24 (42 percent compared to 34 percent of the general population), and a significant percentage of the population falls in the 15-19 age group. Young people are our Nation’s greatest resource, so it is essential that we do everything we can to encourage healthy, drug-free youth communities in Indian Country. One of the conference participants was Margarita, a member of the Ute Mountain Ute Tribal Youth Task Force Coalition, which is a community coalition sponsored by the Drug-Free Communities (DFC) Support Program. This coalition is one of the many examples of how the DFC program is helping to build healthy tribal communities. How has the program grant helped her community? “DFC has played an important role,” said Margarita. “I don’t think the adults know what problems youth are facing because they are not youth anymore. Having young people at the table gives them the advantage to know, ‘okay, this youth said this isn’t a good idea, so maybe we should take a different approach in fighting the battle against substance use.’ ” But it isn’t just about being a voice at the table. Margarita said she also wants “to be the type of role model that people look up to,” and being a role model involves talking to her peers about substance use. Giving her friends “the facts and the statistics of using,” she said, is the best way to illustrate how substance use “will affect their lives in the long run.”The work that Margarita and her group are doing shows how DFC coalitions are positively influencing youth in tribal communities. As Margarita put it, participating in a DFC-sponsored coalition “opens the doors to opportunities that never would have opened before.”To learn more about the Drug-Free Communities Support Program, click here.Learn more about
But it isn’t just about being a voice at the table. Margarita said she also wants “to be the type of role model that people look up to,” and being a role model involves talking to her peers about substance use. Giving her friends “the facts and the statistics of using,” she said, is the best way to illustrate how substance use “will affect their lives in the long run.”The work that Margarita and her group are doing shows how DFC coalitions are positively influencing youth in tribal communities. As Margarita put it, participating in a DFC-sponsored coalition “opens the doors to opportunities that never would have opened before.”To learn more about the Drug-Free Communities Support Program, click here.Learn more aboutCombatting Youth Prescription Drug Use through Coalitions
Posted by on August 5, 2015 at 9:00 AM ESTThis past year, the Concho Valley C.A.R.E.S. Coalition, a Drug-Free Community (DFC) in San Angelo, Texas, pioneered a prescription drug campaign called: Mix it, Seal it, Trash it. The aim of the campaign was to inform adults about the proper procedures for the disposal of unused or expired prescription drugs, which would help prevent youth substance use. So far, the campaign has added two prescription collection units and conducted two prescription drug take back projects.The Concho Valley Coalition is one example of the many ways that DFC coalitions have been taking the lead nationwide in implementing innovative strategies and activities to reduce the misuse of prescription drugs, particularly among youth.In the Drug-Free Community Support Program’s 2014 National Evaluation, we see positive changes in middle and high school youth’s use and perception of prescription drugs. In addition, we can see the progress being made on youth’s use and perception of other substances such as alcohol and tobacco.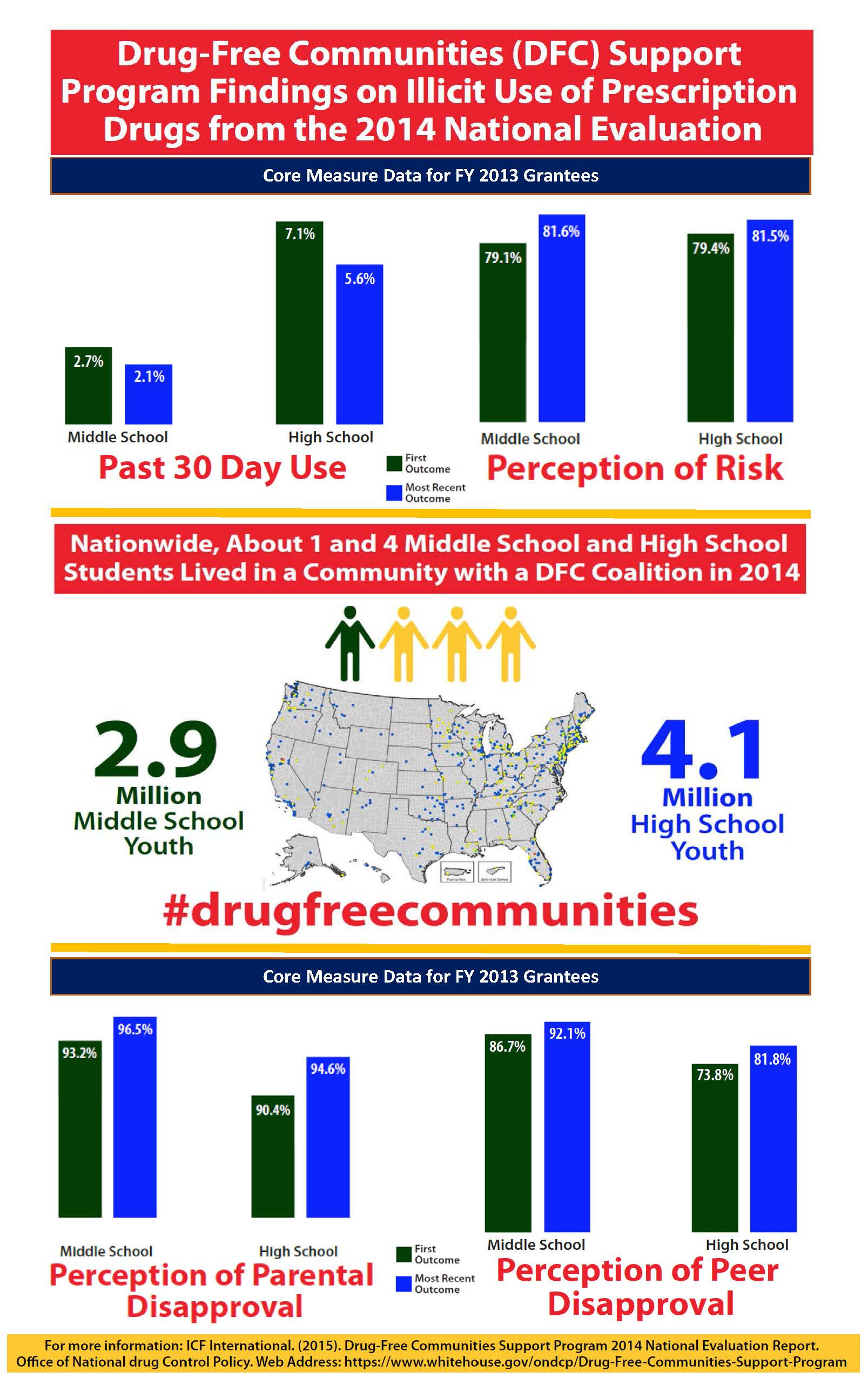 The report shows that across the 618 Drug-Free Communities (DFC) in FY 2013, there are promising results for middle school and high school youth substance use and perception, including
The report shows that across the 618 Drug-Free Communities (DFC) in FY 2013, there are promising results for middle school and high school youth substance use and perception, including- A significant decrease in past 30-day use for alcohol, tobacco, marijuana, and prescription drugs among middle school and high school youth;
- An increase in the percentage of survey respondents who reported that regular use of tobacco, alcohol, or prescription drugs has moderate or great risk;
- An increase in the perception of peer disapproval among middle school students in each of the four substance areas, and for high school students in each substance except marijuana.
- An increase in perception of parent disapproval for each of the substance areas, with the exception of marijuana among high school youth.
It’s clear that coalitions can play an important role in preventing youth substance use. By using a comprehensive, evidence-based approach that engages not only youth, but also parents, teachers, law enforcement, and healthcare providers, these coalitions are helping to protect our nation’s greatest resource: young people.Learn more aboutIn Recognition of World Hepatitis Day
Posted by on July 28, 2015 at 9:50 AM ESTIf we continue to box people in because of their medical conditions, to stigmatize individuals because of their health, and treat diseases as discrete conditions, we will never reach our common goals of health and wellbeing.Michael Botticelli, Director of National Drug Control PolicyToday, as we observe World Hepatitis Day, it is important to consider the relationship between infectious disease and substance use disorders. Both viral hepatitis and HIV can be transmitted by injection drug use; in fact, injection drug use is the major driver of hepatitis C virus (HCV) infections. A recent outbreak of HIV infection in Scott County, Indiana attributed in large to injection drug use behaviors, and increases in HCV infections nationally from 2010 to 2013 underscore the adverse health outcomes of substance use.These outcomes are not inevitable: infectious diseases and substance use disorders are both preventable and treatable. Evidence-based strategies, such as the provision of medication-assisted treatment and integrated screening and treatment service, are needed to better and more comprehensively address the intersection of substance use disorders and viral hepatitis infections to help reduce drug use, bend the curve in HCV infections, and avoid more HIV outbreaks like that in Scott County.HCV infection causes inflammation of the liver and is a major cause of liver disease and cancer. It affects an estimated 3.2 million Americans and studies indicate a high prevalence of HCV among people who inject drugs. HCV can be transmitted by sharing syringes and other equipment used to inject drugs.A number of important advances provide an unprecedented opportunity to address HCV among persons with substance use disorders. These include:- Enhanced access to HCV testing based on the availability of rapid point-of-care tests and US Preventive Services Task Force recommendations for HCV screening among individuals at high risk for infection;
- Improved access to health coverage based on provisions of the Affordable Care Act and Federal parity protections; and,
- New HCV therapies that are effective in curing HCV in the majority of people who complete treatment.
The Action Plan for the Prevention, Care, & Treatment of Viral Hepatitis from the Department of Health and Human Services (HHS) calls for ensuring that persons who inject drugs have access to viral hepatitis prevention, care, and treatment services through the integration of behavioral health and viral hepatitis services. These efforts to prevent and treat HCV infection must be coupled with initiatives that help people who inject drugs get treatment for their substance use disorders, reduce risk of disease transmission from sharing syringes and other injection equipment, and prevent drug use initiation.ONDCP and HHS are committed to reducing the rising rates of HCV infection in the United States. Access to prevention services and treatment should be evidence-based and available to all individuals. An individual’s substance use status should not affect his/her ability to get treatment for HCV infection. Only by ensuring equality and the highest standards of care to all individuals can we be successful in making concrete strides against viral hepatitis.Click here for more information on Hepatitis C prevention and treatment methods.Learn more aboutCelebrating 25 Years of the Americans with Disabilities Act
Posted by on July 24, 2015 at 8:08 AM ESTThis year we celebrate the 25th anniversary of the passage of an historic piece of legislation, the Americans with Disabilities Act (ADA). For the millions of Americans living with a disability, the ADA provides protection from discrimination and guarantees equal opportunities in order to promote accommodations that can help people live full, productive lives. As someone in long-term recovery from a substance use disorder, I strongly share this ideal.
Just as people with physical disabilities benefit under the ADA, people in recovery from substance use disorders are also protected by this landmark legislation. Our communities have a lot in common – we both face some of the same discrimination, stigma, and historical restriction of opportunities. Our shared experience brings us together.
With approximately 56.7 million Americans living with a disability and an estimated 21.6 million Americans living with a substance use disorder, we are a significant portion of the US population.1 2 Despite our numbers, we still face stigma and discrimination in healthcare, education, housing, and employment. The Office of National Drug Control Policy (ONDCP) is working to dismantle the stigma experienced by individuals with substance use disorders, just as the National Council on Disability (NCD) and many others are working to abolish discrimination and stigma surrounding all disabilities. If we combine our numbers, our voices, and our collective experience, we have the opportunity to make our voices heard in all walks of life.
As we celebrate the ADA, let us commit to join forces to address the common challenges faced by our communities. Together, we can work on increasing access to treatment for all people and create a higher standard of care and accommodations through cultural competency training. We can make a significant impact in destigmatizing disability, encouraging compassion and tolerance, and advocating for equality for all persons.
We can carry out that work today, as we celebrate the ADA. But we can also continue that work as we celebrate National Alcohol and Drug Addiction Recovery Month. Each September, ONDCP joins with the millions of people in recovery to observe Recovery Month, and I want to ask you to join the celebration. This year the theme is “Join the Voices for Recovery: Visible, Vocal, Valuable!”
Together, we can join voices to reduce stigma and spread our shared message of effective treatment and successful recovery for anybody with a substance use disorder or disability.
For more resources and to learn more, please visit these links:
1. 2010 Census data, http://www.census.gov/prod/2012pubs/p70-131.pdf↩
2. 2013 National Drug Use and Health Survey, http://www.samhsa.gov/data/sites/default/files/NSDUH-SR200-RecoveryMonth-2014/NSDUH-SR200-RecoveryMonth-2014.htm↩Learn more aboutDrug Policy Reform at Home and Abroad
Posted by on June 26, 2015 at 4:02 PM ESTToday is the International Day Against Drug Abuse and Illicit Drug Trafficking, an annual observation established in 1987 by the United Nations General Assembly. It is an important day to reflect on the progress the world has made against drugs and the many challenges still to be addressed.
One notable example of progress is the increasingly widespread support for a public health-focused approach to the drug problem. Just a few years ago, a focus on prevention, early intervention, behavioral and medication-assisted treatment, overdose prevention, and recovery support services was controversial in many areas of the world. In fact, there was a time when the word “recovery” was not even accepted in U.N. documents. But in 2014, a U.S. resolution on recovery at the annual U.N. global drug meeting (the Commission on Narcotic Drugs) easily won approval. These discussions at the U.N. and elsewhere have led to a greater appreciation of the urgent need to reduce the stigma associated with substance use disorders – both out of genuine compassion and as a means to encourage those who need help to seek treatment.
Implementing public health policies requires a lot of hard work and an investment in building treatment capacity, including training medical professionals on how to address substance use disorders through screening and early intervention. Once medical professionals are trained to screen patients for substance use, they can identify and address problems earlier. This type of assessment can result in huge long-term savings in future criminal justice and other public costs.
Also critical to improving public health is the use of medications to treat addiction and the implementation of medication-assisted treatment (MAT) protocols. Although cultural and social stigmas regarding medications used to treat opioid use disorders persist in some places, clinical research has shown it is highly effective, reducing relapse rates and improving health outcomes significantly.
Another encouraging development is the emerging global consensus in favor of alternatives to incarceration for people with substance use disorders.
There are now over 2,900 drug treatment courts in the United States and dozens more internationally. Over the years, these specialized courts have continued to refine and improve their operations. This intervention has repeatedly demonstrated success in decreasing recidivism, driving drug use down, and reducing criminal justice costs. In addition, DTCs break down the walls that too often divide justice and health agencies, allowing them to work together toward the same goal. It is no surprise that international partners are studying these models and adapting them to the challenges they face in their countries.
In just over a decade, Hawaii's Opportunity Probation with Enforcement (HOPE) and similar initiatives operating in about 40 jurisdictions have helped to inspire probation reforms across the United States. The Swift, Certain, Fair approach reduces drug use, recidivism, and crime by employing brief, consistently applied sanctions for every probation violation. Treatment is provided to those who request it. An independent evaluation of the HOPE program found that participants – primarily methamphetamine users – were 55 percent less likely to be arrested for a new crime; 72 percent less likely to use drugs; 61 percent less likely to skip appointments with their supervisory officer; and 53 percent less likely to have their probation revoked.[1]
As the international community prepares for the U.N. General Assembly Special Session on drugs in April 2016, the United States will advocate wider adoptions of vital reforms such as these around the world.
More information about medication-assisted treatment and alternatives to incarceration is available at http://www.dpt.samhsa.gov, the National Association of Drug Court Professionals, and the SwiftCertainFair Resource Center.
[1] “Swift and Certain” Sanctions in Probation are Highly Effective: Evaluation of the HOPE Program, Office of Justice Programs, National Institute of Justice. Available at: http://www.nij.gov/topics/corrections/community/drug-offenders/pages/hawaii-hope.aspx
Learn more aboutHow Drug Courts Make the Case for Alternatives to Incarceration
Posted by on May 27, 2015 at 10:44 AM EST
Director Botticelli with drug court graduate Donovan Simmons.
Donovan Simmons was the type of person many judges might have written off. He had pled guilty to a series of criminal charges, including burglary, and had been sentenced to five years in prison.
But Judge David Tapp of Somerset, Kentucky, refused to write Donovan off.
Like many people who come into contact with the criminal justice system, Donovan had a long history of substance use disorders. He struggled with serious marijuana and opioid use disorders, which began as he tried to cope with childhood trauma. Donovan was ill and needed medical treatment, not jail.
For decades, science has shown that addiction is a chronic brain disease—not a moral failing on the part of an individual. So treating the disease can give people caught up in the criminal justice system a chance to break free from the cycle of drug use, crime, arrest and imprisonment.
Learn more aboutCommunity Policing and Drug Overdose: Where You Live Doesn't Have to Determine Whether You Survive an Overdose
Posted by on May 19, 2015 at 12:50 PM ESTThe odds of surviving a drug overdose, much like the odds of surviving a heart attack, depend on how quickly the victim receives treatment. But access to naloxone—which can reverse heroin and prescription drug overdoses--varies greatly across the country, even though all drug poisoning deaths have surpassed traffic crashes as the most lethal cause of preventable injury. Because police are often the first on the scene of an overdose, the Obama Administration has strongly encouraged local law enforcement agencies to train and equip their personnel with naloxone.
Yesterday, the President traveled to Camden, New Jersey, a city that’s taken steps to create economic opportunity, help police do their jobs more safely, and reduce crime in the process. Yet another area where the Camden County Police Department is taking the right steps is with its creation of an overdose prevention program. This program has reversed 68 overdoses since it started a year ago. Across New Jersey, law enforcement officers have used naloxone to respond to overdoses 888 times since 2014.
By engaging with law enforcement in naloxone administration, we are truly pursuing a 21st century approach to drug policy and community policing--one that combines public health with public safety.
Recently I met Corporal Nicholas Tackett, a police officer from Anne Arundel County in Maryland. Corporal Tackett has witnessed about 50 drug-related overdoses in his law enforcement career.
He knows the signs of overdose, the looks on their faces. Now, with naloxone, he has a tool that enables him to save lives. Corporal Tackett brought me to the locations where his use of naloxone reversed the life-threatening overdoses of two people. Naloxone works, and it is an incredibly important tool.
In October 2014, the Department of Justice released a Naloxone Toolkit for law enforcement. This toolkit is an online clearinghouse of more than 80 resources, such as sample policies and training materials designed to support law enforcement agencies in establishing a naloxone program.
In the past year, we have witnessed an exponential expansion in the number of police departments that are training and equipping their police officers with naloxone. They now number in the hundreds and they are saving lives.
The Police Department in Quincy, Massachusetts, has partnered with the State health department to train and equip police officers to resuscitate overdose victims using naloxone. The Department reports that since October 2010, officers in Quincy have administered naloxone in more than 382 overdose events, resulting in 360 successful overdose reversals.
The Vermont Department of Health has been distributing Overdose Rescue Kits with naloxone to State police as well as to individuals through community-based partners. To date, naloxone has been deployed 146 times across the State.
There is also collaboration taking place in rural and suburban communities. In Illinois, the Lake County State’s Attorney has partnered with various county agencies, including the Lake County Health Department; drug courts; police and fire departments; health, advocacy and prevention organizations; and local pharmacies to develop and implement an opioid overdose prevention plan. As of February 2015, the Lake County Health Department had trained 828 police officers and 200 sheriff’s deputies to carry and administer naloxone, and more departments have requested this training.
To build on these efforts, the President’s FY 2016 Budget directs the Department of Health and Human Services to permit the use of block grant funds for naloxone purchases. It also provides funding specifically for law enforcement to purchase naloxone.
Where you live shouldn’t determine whether or not you survive an overdose. So our goal is to get naloxone in every community where overdose deaths are prevalent. Combined with evidence-based prevention programs and access to effective treatment, this approach will save the lives of many Americans.
Michael Botticelli is Director of National Drug Control Policy.
Learn more aboutHonoring Courage and Saluting Sacrifice During National Police Week
Posted by on May 15, 2015 at 5:00 AM ESTThis week, Director Michael Botticelli joins thousands of law enforcement officers from across the country, President Obama, Attorney General Loretta Lynch, Secretary Jeh Johnson and other distinguished officials in Washington, D.C. to honor the lives of officers who have gave the ultimate sacrifice.
As part of National Police Week, Director Botticelli read the names of three fallen officers at the 27th Annual Candlelight Vigil at the National Law Enforcement Officers Memorial. Today, he will join President Obama at the 34th Annual National Peace Officers’ Memorial Service on the West Front Lawn of the United States Capitol.
Law enforcement officers have a profound sense of duty to serve and protect their communities. Every day, they place their lives on the line knowing they could be exposed to harm at any moment. ONDCP honors all the brave men and women who have died to protect the safety of others.
During Police Week, we also particularly recognize officers on High Intensity Drug Trafficking Area (HIDTA) Task Forces who, despite the risks, remained steadfast and gave their lives in the line of duty, including Ogden Police Officer Jared D. Francom, Los Angeles Sheriff's Department Deputy Sheriff Jerry Ortiz, Glendora Police Detective Louis Pompei
,FBI Special Agent Paul M. Sorce and Maryland State Police Corporal Edward M. Toatley.We owe all those who we have lost, and the men and women keeping us safe today, our deepest gratitude for protecting our families, homes and communities.
Learn more aboutThe Indianapolis Star: "Work to prevent opiate drug abuse"
Posted by on May 4, 2015 at 4:56 PM ESTSince Gov. Mike Pence issued a public health disaster emergency order in response to the state's HIV outbreak, public and private leaders have marshalled a remarkable effort to identify cases, provide care and support to those who have tested positive for HIV, and prevent new infections. This evidence-based approach is critical to effectively contain the outbreak.Last fiscal year, the federal government invested more than $23.2 million to support HIV, sexually transmitted disease and viral hepatitis prevention, treatment and response activities in Indiana. Federal-state partnerships like this are essential to achieving an AIDS-free generation.Learn more aboutWe Don’t Have Time to Wait
Posted by on April 21, 2015 at 9:29 AM ESTThis is a picture of Taylor Smith from Holly Springs, Georgia, with her sister, Gabrielle.

Taylor Smith (right) with her sister, Gabrielle Smith.
Taylor died of an overdose.
Her mother, Tanya Smith, writes:
"Taylor was a freshman, junior varsity and varsity squad basketball and football cheerleader at Creekview High School; known for her quick wit and infectious squeaky laugh, she was an avid animal rescuer, and quickly came to the defense of those she felt were treated unfairly. She was 20 years old when she overdosed in the company of friends, who subsequently dumped her body in the yard of an abandoned trailer to avoid arrest for drug possession.”
Taylor might still be alive if her friends had known that Georgia, along with 21 other states and the District of Columbia, has legal protections in place that shield people possessing drugs from criminal liability if they’re helping someone having an overdose.
Her mother Tanya has channeled her grief into action, pushing to make sure that law enforcement officers in her town now carry naloxone — the antidote for opioid overdose.
Learn more about