ONDCP Blog
What Drug Policy Reform Looks Like
Posted by on February 25, 2013 at 12:30 PM ESTPresident Obama believes in the pursuit of an America built to last – a Nation founded on an educated, skilled workforce with the knowledge, energy, and expertise to succeed in a highly competitive global marketplace. Yet, for too many Americans, this vision is hampered by drug use and addiction, which inhibits their ability to live healthy lives and achieve their full potential.
While the harms caused by substance use and substance use disorders may seem obvious, here’s a reminder of what the data show: According to the CDC, drug overdose deaths are the second leading cause of injury death, surpassed only by suicides. Making matters worse, studies show that among the 22 million Americans who need treatment for substance use disorders, only about 2 million—only about one-in-10—receive it [i]. What has caused this disparity? For a start, not all health insurance plans have been required to cover drug treatment on par with other medical problems. That’s unacceptable.
This week, the Obama Administration announced a major milestone in drug policy reform that builds on our record of treating drug use as a public health, not just a criminal justice issue. Through a new rule made possible by the Affordable Care Act, we are requiring insurers to treat substance use disorders in the same way they would any other chronic disease. Specifically, this new rule expands coverage of mental health and substance use disorder services to 62 million Americans. In today’s heated debate over drug policy, it is worth noting that this is one of the most significant pieces of drug policy reform in a generation.
Why does this matter? Practitioners in our health care system historically have not screened for substance use disorders and often have limited knowledge of the nature of addiction. As a result, significant resources are spent treating the symptoms of Americans with undiagnosed substance use disorders. Research shows that treating substance misuse before it develops into a chronic disease is the best course of action. Implementing screening and brief intervention protocols has shown to be effective in reducing problematic substance use and its consequences. For those who have already developed an addictive disorder, only 10 percent of the population who need treatment receive it—often because of insufficient insurance coverage.
Like most chronic diseases, a substance use disorder is progressive. As it progresses, it changes the brain, leading to ever more damaging consequences and making the disease more difficult to treat. If we can ward off problematic substance use before an addictive disorder develops, we can prevent the disease’s most serious consequences. Treatment makes good financial sense as well. Because for every dollar we spend on treatment, we realize a benefit of seven dollars as a result of reduced criminal justice system costs and increased employment earnings. [ii] That means less incarceration, safer communities, healthier citizens, and a stronger workforce.
The most important thing we can do to reform our drug policies is to change the way we think about – and address -- our Nation’s drug problem. A "war on drugs” should not define how we can make America healthier and safer. We cannot arrest our way out of the drug problem. So while smart law enforcement efforts will always play a vital role in addressing drug related crime in America, we must acknowledge that science shows addiction is a disease of the brain that can be successfully prevented and treated.
That is why equal access to drug treatment programs is a priority for this Administration. After all, treatment should not be a privilege limited to those who can afford it, but a right available to all those who need it. That is what real drug policy reform looks like.
[i] In 2010, an estimated 23 .1 million Americans (9 .1 percent ) aged 12 or older needed specialized treatment for a substance use disorder, but only 2 .6 million (or roughly 11 .2 percent of them) received it .
[ii] 37 . Ettner, S . L ., Huang, D ., Evans, E ., Ash, D . R ., Hardy, M ., Jourabchi, M ., & Hser, Y . I . (2006) . Benefit-cost in the California treatment outcome project: Does substance abuse treatment ‘pay or itself’? Health Services Research, 41(1), 192-213
Learn more aboutDebunked: Claim that Young People Find it Easier to get Marijuana than Alcohol
Posted by on February 22, 2013 at 2:40 PM ESTThe independent, non-partisan fact-checkers at Politifact have tackled another claim frequently made in today’s debate about drug policy. The claim goes something like this:
“Despite laws outlawing certain drugs, young people still find it easier to get marijuana than alcohol.”
If that seems implausible to you, that’s because it is. According to PolifiFact:
“…all the most recent, credible, national studies we found showed that teenagers report it’s easier to get alcohol than marijuana.”
You can read their full reporting here.
This is part of a series of blog posts that address myths about federal drug policy. See also:
Are Drugs Today Really Cheaper, Purer, and More Available Than Ever?
Drug Laws: Why Do We Have them, and Do They Work?
Learn more aboutToward a Smarter Drug Policy
Posted by on February 14, 2013 at 11:14 AM ESTPlease note that this is a co-authored blog post by Gil Kerlikowske, Director, ONDCP and Benjamin Todd Jealous, President and CEO, NAACP. This post also appears on The Huffington Post and the NAACP blog.
In Los Angeles not long ago, a man named Michael Banyard ran afoul of California’s “three strikes” law. After bouts of homelessness, unemployment, suicidal thoughts, and a criminal record driven by an underlying substance use disorder, Michael faced a mandatory 25-year prison sentence.
Fortunately for Michael, Federal District Court Judge Spencer Letts was put in charge of his final sentence appeal. Judge Letts saw Michael not as a hopeless, drug-using criminal, but as an individual with a disease in need of help. The judge then did something highly unusual. He not only reversed Michael’s sentence, he invited him into his chambers to talk.

Here were two men who could not be more different – a white, Yale- and Harvard-educated judge and former corporate vice president, and a shy African American who had spent most of his adult life in prison. And yet, the men found they had more in common than either could have imagined. Judge Letts knew that repeatedly incarcerating Michael wasn’t accomplishing much.
Over the years, Judge Letts became, in Michael’s words, the father he never had. The Judge gained something extraordinary too. Michael, he said, “showed me that my gut feeling was right – that people are basically the same, with the same basic goodness, if you just give them the chance.” Today, Michael Banyard has received his GED degree and spends his time volunteering at the Los Angeles Dream Center, where he graduated from a faith-based program that he credits for his transition away from substance abuse.
Stories like this illustrate the kind of thinking needed to reform our nation’s criminal justice and drug control policies. In 2011, about seven million people were under the supervision of the criminal justice system in the United States. Of these, about two million were behind bars. And nearly one quarter - 500,000 - of those behind bars are there for drug related offenses. America’s incarceration rate – 756 per 100,000 population – is the highest in the world. High rates of incarceration have resulted in prison overcrowding and state governments facing the costs of a rapidly expanding penal system.
In addition, our nation’s historical emphasis on incarceration has significantly affected communities of color. African Americans are disproportionately incarcerated for drug offenses, accounting for almost half (45 percent) of all drug offenders in state prison in 2010. (Whites accounted for 29 percent.) Among prisoners age 18 to 19, African American males are imprisoned at more than 9 times the rate of white males, and African American females are imprisoned at between 2 and 3 times the rate of white females.
It is clear that we cannot simply arrest our way out of the drug problem. Instead, we need smarter, results-based criminal justice policies to keep our communities safe, including treatment for people with substance use disorders and mental health issues.
To bring about real, meaningful change, we need a fundamental shift in how our Nation discusses drug policy. This begins with the acknowledgement that our drug problem is a public health issue, not just a law enforcement issue. It means acknowledging that an ever-growing body of scientific research clearly demonstrates that addiction – the underlying cause of too much crime in this country – is a disease that can be prevented and treated successfully.
Armed with the indisputable fact that preventing and treating addiction is an effective strategy for reducing substance abuse and crime, the Obama Administration and the NAACP are committed to pursuing evidence-based policies that strengthen families and communities across America.
Already, the Administration has worked to expand specialized courts that divert roughly 120,000 non-violent offenders into treatment instead of prison each year. The President has requested that Congress increase its commitment for drug treatment programs for 2013. And in 2010, President Obama signed into law the Fair Sentencing Act, which made progress in reducing the 100-to-1 disparity between sentences for powder and crack cocaine that disproportionately affected minorities and also eliminated the mandatory minimum sentence for simple possession of crack cocaine.
Significant accomplishments all, yet more must be done, particularly at the state level.
Demonstrating how criminal justice reform can be a bipartisan issue, the NAACP has worked tirelessly with elected officials from both parties to achieve sensible reform. With the support of the NAACP, Republican Governor Nathan Deal of Georgia signed into law the most sweeping criminal justice reform legislation in the country. The NAACP also worked to find common ground with Republican Governor Bob McDonnell of Virginia, who shut down prisons and called for more money to be sent to universities. In Texas, the NAACP helped push Republican Governor Rick Perry to sign 12 progressive reforms that led to Texas scheduling the first prison closure in the state’s history.
Actions by the Obama Administration, the NAACP, and others are vital steps toward reshaping and redirecting our nation’s criminal justice system. These are only the first steps, however, and the road ahead is long. It will take still more action, more time, more work, and more innovative thinking to bring about the reforms that are so urgently needed.
The challenge is immense, but America is up to it. Working together, we can reduce the heavy toll of substance use in our cities, neighborhoods, and families. Combining proven public health and public safety strategies will help break the vicious cycle of drug abuse, crime, and incarceration. This, in turn, will save countless lives and taxpayer dollars, make America stronger and safer, and ensure a more perfect union.
It’s not only the right thing to do—it’s the smart thing to do.
Learn more aboutGuest Post: Helping Youth and Turning Lives Around through Education
Posted by on February 13, 2013 at 12:46 PM ESTThroughout my career as a law enforcement officer specializing in juvenile issues, I have seen first-hand the consequences of drug use on our young people. Drugs can ruin lives and lead to a multitude of other problems, such as school apathy and low self-esteem. This creates an endless cycle.
But I have also seen the success of drug prevention programs in schools. As a former president of Lions Clubs International, former chairman of Lions Clubs International Foundation, and a current member of the Lions Quest Advisory Committee, I have visited classrooms and spoken with teachers who use our materials. Through its programs and materials, Lions Clubs International teaches respect of self, respect for others, and rejection of bullying, and it delivers a strong message to young people about the dangers of drug and alcohol use.
Because drug use knows no age, gender, race, or socioeconomic boundaries, we at Lions Clubs International know we have to share solutions with partner organizations. I have met with elected officials and helped coordinate partnerships with a number of government and non-governmental organizations – including Community Anti-Drug Coalitions of America, the Organization of American States Inter-American Drug Abuse Control Commission, the United Nations Office of Drugs and Crime, and the State Department’s Bureau of International Narcotics and Law Enforcement – in an effort to reach classrooms around the world and in my home State of New York. Today, our materials are used more than 70 countries. Our middle school program is listed on the National Registry of Evidence-Based Programs and Practices, and in the Department of Education's guide to Exemplary & Promising Safe, Disciplined, and Drug-Free Schools Programs. Why? Because it works.
Lions Club International helps turn lives around and lead young people along the path to success. Our educational programs are just one part of Lions Clubs International’s global long-term commitment to youth and drug abuse prevention. If we are not giving our young people the tools they need to succeed and the wherewithal to say “no” to drugs, we are doing them a grave disservice. Education is one of the best tools available for ensuring our youth make intelligent decisions that help them stay happy, healthy, and drug free.
 Learn more about
Learn more aboutAre Drugs Today Really Cheaper, Purer, and More Available Than Ever?
Posted by on February 12, 2013 at 1:41 PM ESTYou’ve probably heard this claim: Despite decades of effort, we’ve failed to make any significant progress in reducing drug use in this country. Some critics go so far as to say that “illegal drugs are cheaper, purer, and more available today” than ever before. This is a compelling argument and a powerful sound bite, to be sure. There’s just one problem:
It’s not true.
While gaining a clear picture of the illegal drug market is always a challenge, a vast array of data, research, and surveys reveal long-term trends and shed valuable light on the nature and scope of the drug problem in America. The evidence presented by these sources is vital in our work to meet the President’s mandate of promoting policies grounded in science and research.
So what do the data show? Simply put, our national drug problem is substantially smaller than it used to be, and progress continues to be made.
Here’s the evidence:
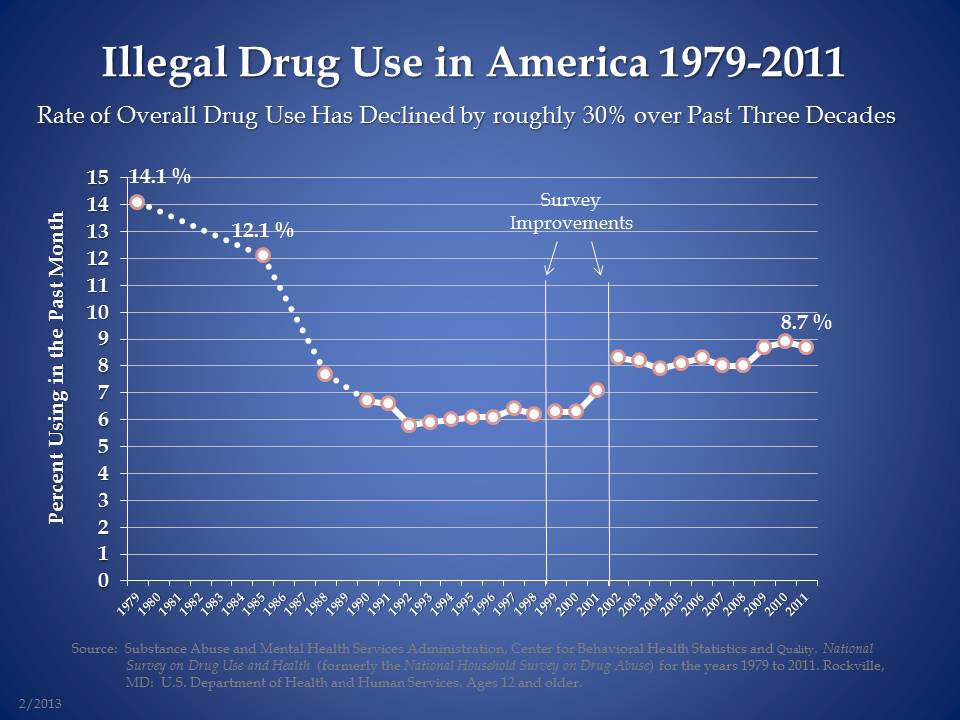
- According to the National Survey on Drug Use and Health – the Nation’s largest, longest-running, and most comprehensive survey on drug use – the overall rate of drug use in America has dropped by roughly 30 percent over the past three decades.
- More recently (since 2006), the number of past month (current) users of any illicit drug other than marijuana has dropped 16 percent. Driving this decline have been decreases in the number of current users of cocaine (44 percent), meth (40 percent), and prescription drugs (14 percent).
- The Monitoring the Future study, the most important youth survey on drug use in America, has shown that the overall rate of illicit drug use among high school seniors has fallen by 35 percent since 1979.
- The same survey of youth drug use reports that the perceived availability of cocaine among high school seniors has dropped by nearly 50 percent since its peak in 1989.
- According to STRIDE (System to Retrieve Information from Drug Evidence) – law enforcement’s largest forensic laboratory database – cocaine purity over the past few years dropped to levels not seen since reporting began in 1981, indicative of a significant disruption in the U.S. cocaine market. In response, the number of current cocaine users in 2011 dropped significantly from levels in 2002 through 2008.
- According to the United Nations, “cocaine consumption has fallen significantly in the United States in the past few years. The retail value of the US cocaine market has declined by about two thirds in the 1990s, and by about one quarter in the past decade.”
- According to the Center for Disease Control and Prevention’s National Center for Health Statistics, unintentional overdose deaths in the U.S. related to cocaine dropped 41% from 6,726 in 2006 to 3,988 in 2009, the year for which the most recent data are available.
- Cocaine production in Colombia – the source of most cocaine consumed in America – has plummeted by over 70 percent since 2001.
Again, these facts are proof that we are not powerless against the drug problem in America. As the President himself has noted, we have successfully made a difference in other areas, like smoking and drunk driving, so there’s no reason to think we cannot continue to achieve the same success with illegal drugs. Our challenge, it’s worth pointing out, is not that we are unable to reduce drug use; indeed, we have made great strides in that effort. The challenge is that rates of drug use are still too high.
Drug use and its consequences continue to place too many obstacles in the way of young people working to achieve their full potential. It still drives violent crime in our neighborhoods, in our cities, and throughout our hemisphere. It still fosters substance use disorders that tear families apart and end too many lives. This Administration will continue working aggressively to address this challenge in a smart and comprehensive way, and with a clear and realistic goal: to reduce drug use and its consequences by 15 percent over the next five years.
We are energized by the ongoing national debate about drug policy reform in America. That’s why we’ve put forth a National Drug Control Strategy that outlines more than 100 specific drug policy reforms that build on the progress we have made thus far. Still, as we engage in this important national conversation about how best to protect public health and safety in America, we must remain focused on using science and research – not ideology or dogma – as our guide in this national discussion.
This is part of a series of blog posts that address myths about federal drug policy. Related: Independent fact checkers at Politifact dispel claim that marijuana is easier for young people to get than alcohol.
Learn more aboutWatch Dr. Nora Volkow Explain How Neuroscience Shapes Drug Policy
Posted by on February 11, 2013 at 4:01 PM ESTWatch Dr. Nora Volkow describe the scientific foundation for Federal drug policy:
The National Institute on Drug Abuse and the Office of National Drug Control Policy agree that throughout much of the last century, scientists studying drug abuse labored in the shadows of powerful myths and misconceptions about the nature of addiction. When science began to study addictive behavior in the 1930s, people addicted to drugs were thought to be morally flawed and lacking in willpower. Those views shaped society's responses to drug abuse, treating it as a moral failing rather than a health problem, which led to an emphasis on punitive rather than preventative and therapeutic actions.
Today, thanks to science, our views and our responses to drug abuse have changed dramatically. Groundbreaking discoveries about the brain have revolutionized our understanding of drug addiction, enabling us to respond effectively to the problem.
As a result of scientific research, we know that addiction is a disease that affects both brain and behavior. We have identified many of the biological and environmental factors and are beginning to search for the genetic variations that contribute to the development and progression of the disease. Scientists use this knowledge to develop effective prevention and treatment approaches that reduce the toll drug abuse takes on individuals, families, and communities.
Learn more aboutDrug Laws: Why Do We Have them, and Do They Work?
Posted by on February 5, 2013 at 3:39 PM ESTIt’s a question often raised in today’s heated discussion about the efficacy of drug policy in America: Do regulations outlawing certain drugs actually work?
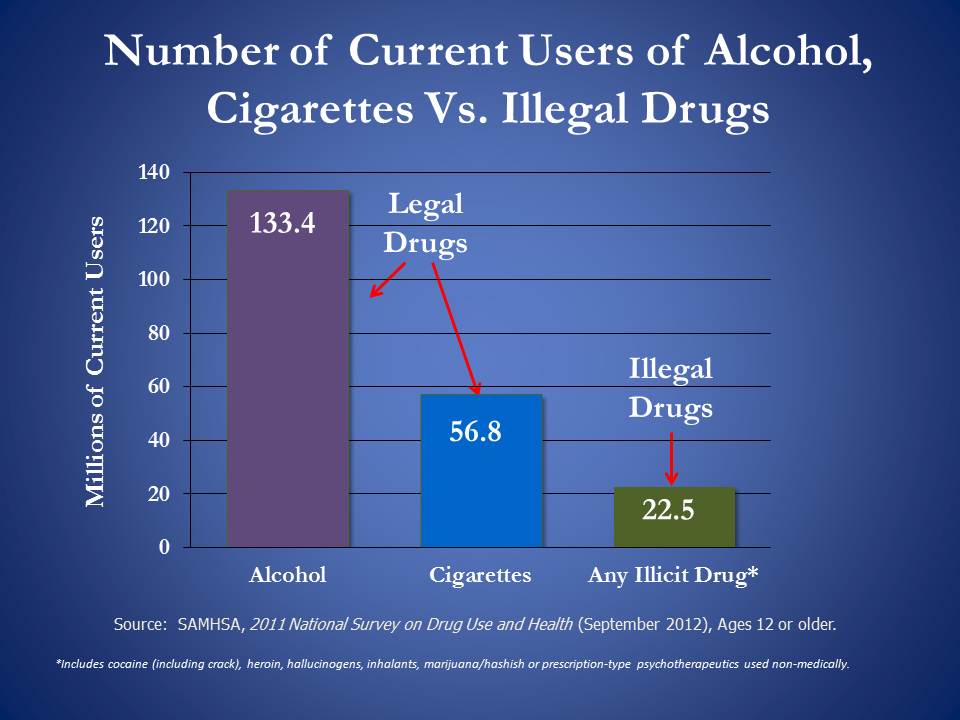
Let’s go to the data. Here’s what the Nation’s largest, longest-running, and most comprehensive source on the state of drug use in America shows:
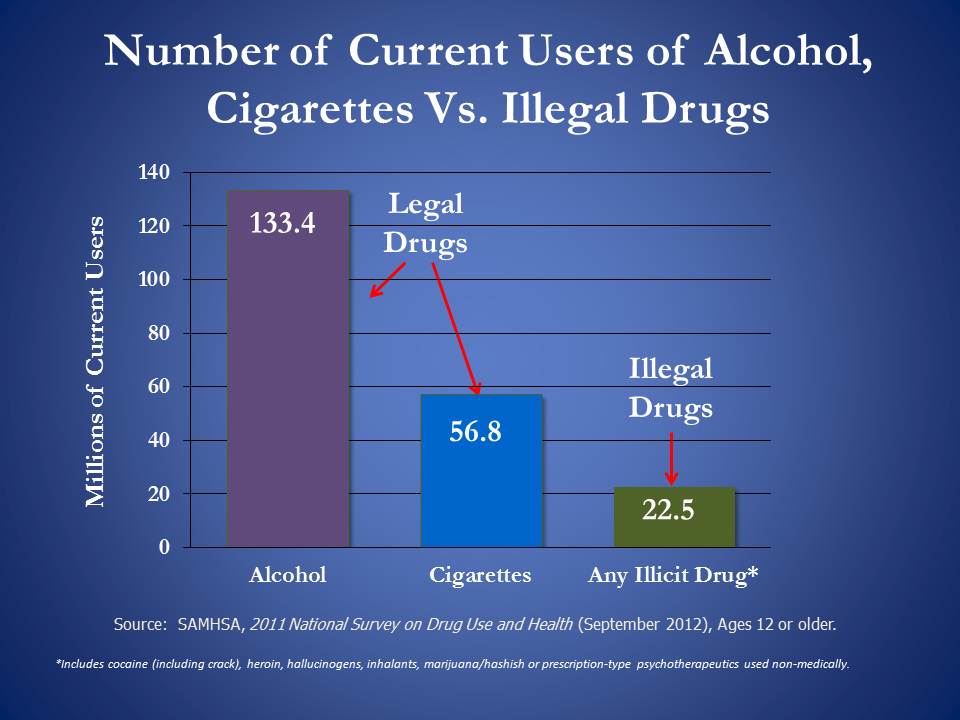
As you can see, the use of legal drugs like alcohol and tobacco far outpaces the use of illegal drugs. It is clear, then, that laws discouraging drug use do have an effect in keeping rates relatively low compared to rates for other drugs that are legal and therefore more available. Even beyond this one-year snapshot, we know that significant progress has been made in the long term. Since 1979, there has been a roughly 30 percent decline in the overall use of illicit drugs in America. . (Related: Independent fact checkers at Politifact dispel claim that marijuana is easier for young people to get than alcohol.)
So our challenge is not that we’re powerless against the problem of substance use in America. The challenge is that rates of drug use – a behavior that harms too many of our fellow citizens -- are still too high. That’s why the President’s National Drug Control Strategy supports innovative and proven programs that aim to reduce drug use and its consequences through a combination of public health and public safety interventions.
It boils down to simple arithmetic: The more Americans use drugs, the higher the health, safety, productivity, and criminal justice costs we all have to bear. And if sensible drug laws (in combination with a wide array of prevention, treatment, and other health interventions, of course) help keep those numbers down, then the answer is yes, they are working.
This is part of a series of blog posts that address myths about federal drug policy. Related: Are Drugs Today Really Cheaper, Purer and More Available than Ever?
Learn more aboutGuest Post: Michael Banyard’s Story, Part 1.
Posted by on January 31, 2013 at 12:50 PM ESTIn June 2012, National Drug Control Policy Director Gil Kerlikowske visited the Betty Ford Center, one of the Nation’s oldest and most recognized addiction treatment facilities. There he gave remarks to a crowd of leaders in the field of recovery. In the audience were two special guests—Michael Banyard and Federal District Court Judge Spencer Letts. In his remarks, Director Kerlikowske mentioned Banyard’s improbable—and inspirational—journey from crack cocaine dependence and homelessness, to prison, to a successful sentence appeal, to the chambers of a federal district court judge and completion of his GED.
Michael Banyard has graciously shared his story—in his own words—with ONDCP, which we are posting in conjunction with National Mentoring Month. Please find the first installation of Michael’s story below.
I was a young man born in Compton, California and raised by a single loving mother. I made a lot of bad decisions; even though my mother raised me right and worked hard to make sure I always had a roof over my head and food on the table.
Michael Banyard in his youth (Photo courtesy of Michael Banyard).
Although I had my mom and two sisters, I still felt alone and would play by myself a lot. I was the only male in the house and felt like I was missing a father figure, so I began looking for guidance outside my home.

Obie Chappell, Michael's mother (Photo courtesy of Michael Banyard).
It was around the age of 12 that my mom started taking me to church. By then, I had already smoked my first joint and had my first drink of alcohol. Around the age of 16, I stopped going to church and went after what I thought I was missing in my life. This led me to a lot of negativity.
My drug and alcohol use got worse, and I became completely detached from school. In 1985, I finally dropped out, and during that same year, I smoked crack cocaine for the first time.
Crack cocaine took my life to another level. I always thought drugs were for fun, but I had no idea it would lead to making me homeless and would have my mind focused on drugs every second of every day. From 1987 to 1995, I ended up in prison five times, and was already in my first four drug programs. Also in that period, I became homeless for the first time. And by 1996, I went back to prison and was convicted of possession and sentenced under the California "Three Strikes" law to a whopping term of 25 years to life.
I was sent to a high security prison called Pelican Bay. While at Pelican Bay, another lifer had one day told me, "You won't feel the life sentence until after your first 10 years." Even though I had been to prison before, I could not see myself behind bars for ten years straight.
After a couple years my custody points dropped, and I became a level three inmate and was allowed to transfer to a lower level three yard. I relocated to Lancaster State Prison in L.A. County.
Michael during his incarceration, facing a 25 year-to-life sentence under California's "Three Strikes" law (Photo courtesy of Michael Banyard).
While at Lancaster Prison I became the G.E.D. Clerk, and while working one day, I overheard the correctional officer talking to her workers. She said, "The sun rotates, and while the sun is rotating, the earth is rotating around the sun, and while that is happening the moon is rotating around the earth."
When I pictured that in my head I thought to myself, "Whoever is in control of that has the last say on whether I spend the rest of my life in prison."
After work I got on my knees and had a long talk with God. The first thing I felt I had to do was take responsibility for the role I played in my situation. Second, whoever I felt may have wronged me, I had to inwardly forgive them before I could move on.
That inner freedom allowed me, a high school drop-out, to start going to the Prison Law Library and studying for the first time.
Note: This is Part 1 of the Michael Banyard guest blog post series. Read Part 2 here.
Learn more aboutTransportation Safety Leader Prioritizes Drugged Driving Prevention
Posted by on January 30, 2013 at 2:28 PM ESTAmericans are well aware of the dangers associated with drunk driving. Thanks to a public awareness campaign spanning decades and driven by a spectrum of government and private organizations, both public perception and the criminal justice system have moved to decrease the rate of driving under the influence of alcohol.
However, drugged driving is now emerging as a growing problem in America. ONDCP, in partnership with the Department of Transportation (DOT) and other federal agencies, has been working to raise awareness about—and prevent—drugged driving.
We are encouraged that last week, the National Transportation Safety Board (NTSB) announced that drugged driving is one of its advocacy priorities for 2013. From the NTSB website:
More people die on the highways than in any other mode of transportation. In fact, over 90 percent of all transportation-related deaths occur on highways. Unfortunately, the substance-impaired driver greatly contributes to this average. For example, in 2010, more than 10,000 deaths (30 percent of all highway deaths) involved an alcohol-impaired driver. Over the last decade, 130,000 people have died in crashes involving an alcohol-impaired driver—20,000 more than the number of seats at the University of Michigan football stadium! According to the 2011 Traffic Safety Culture Index of the AAA Foundation for Traffic Safety, over 14 percent of drivers admit to driving when they thought they were close to or over the legal limit.
The statistics for drugged driving are no less concerning. According to the 2009 National Survey on Drug Use and Health, roughly 10.5 million people age 12 and above admitted to driving while impaired by illicit drugs. And among drivers fatally injured in 2009 who were tested for drugs and for whom results were known, one-third tested positive. From 2005-2009, the proportion of fatally injured drivers who tested positive for illicit drugs rose from 13 to 18 percent. The battle against substance-impaired driving is far from over.
Learn more aboutDoes Drug Treatment Work?
Posted by on January 30, 2013 at 10:30 AM ESTAddiction is a chronic disease that can be successfully treated. We need to look no further than the millions of Americans who are in long-term recovery today from drug and alcohol addiction to see that recovery is possible. Still, there remains some cynicism about the efficacy of drug treatment, and some people claim that the chances of treatment succeeding are very low. In actual fact, relapse rates for drug-addicted patients are about the same for other chronic illnesses.
According to the National Institutes of Health:
“Does relapse to drug abuse mean treatment has failed?
No. The chronic nature of the disease means that relapsing to drug abuse is not only possible, but likely. Relapse rates (i.e., how often symptoms occur) for drug addiction are similar to those for other well-characterized chronic medical illnesses such as diabetes, hypertension, and asthma27, which also have both physiological and behavioral components. Treatment of chronic diseases involves changing deeply imbedded behaviors, and relapse does not mean treatment failure. For the addicted patient, lapses back to drug abuse indicate that treatment needs to be reinstated or adjusted, or that alternate treatment is needed.
Source: JAMA, 284:1689-1695, 2000
Relapse rates for drug-addicted patients are compared with those suffering from diabetes, hypertension, and asthma. Relapse is common and similar across these illnesses (as is adherence to medication). Thus, drug addiction should be treated like any other chronic illness, with relapse serving as a trigger for renewed intervention.27
Learn more about
{kind=link}
- &lsaquo previous
- …
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- …
- next &rsaquo